

The Year of Merciless Killing
A Canadian scientist argues that a recurring spike in Covid deaths around the globe betrays a pattern of mass homicide due to government policy bearing down on care homes.


Anyone who has been observing the roll-out of the Covid-19 scam must give the devil his due: This is the biggest and most spectacular confidence trick ever perpetrated. Even if you describe it with minimum sensationalism, it remains sensational: That a nondescript ‘flulike’ virus (its custodians’ own description) was weaponised to subdue the human inhabitants of the formerly Free World, strip them of their rights and freedoms, destroy their livelihoods and terrify them to the point that they would do almost anything to become immune to a ‘deadly disease’ that was at worst the equivalent of a mid-range influenza. You have to take your hat off to that.
But what if it were even more spectacular than even that? What if there were not merely no pandemic, but actually no disease, no ‘novel’ virus, or at least no single ‘novel’ virus? What if, instead of merely weaponising a new and relatively benign pathogen, the plotters had weaponised instead the normative pathogenic attrition of an average year, with (perhaps) a minor newcomer thrown in, secure in the knowledge that most people have no idea how many people die at any particular point on the calendar, or of what? What, then, to do with your hat?
There is a plausible case, and some very convincing evidence, that something very close to this is what happened. In fact, it is the only explanation that makes total sense of what we have observed play out across the world since the early spring of 2020.
Firstly, it is now well established — in all but ‘official’ (i.e. corrupt) media circles and sources — that the PCR test used to detect potential infections is wholly unreliable, unfit for purpose and subject to an 80%+ rate of false positive. Many scientists have emerged to confirm that no virus conforming to the unique personality attributed to SARS-CoV-2 can be identified in isolation by the PCR test commonly in use around the world and in Ireland under the auspices of the HSE. It is also the case that the US Center for Disease Control and Prevention (CDC), the UK Department of Health, and latterly the HSE, have admitted that no isolates of the SARS-CoV-2 virus, nor any publications confirming such isolation, are in existence. If, according to these authorities, the virus is not scientifically identifiable, how then can it be vaccinated against?
There has also, from the beginning, been ubiquitous evidence of massive massaging of fatality figures to make it appear that Covid is responsible for many deaths of which it is merely, if anything, an accompanying factor.
The weirdest thing about all this information is that it has been in the public domain since last spring, and yet has not penetrated the public consciousness as a game-changing factor. This is largely due to the sneaky way such material is ‘reported’ (when it is) by legacy media, which refer to it in a fashion that suggests it is of no consequence to the meanings at play in the Covid saga.
A Canadian scientist called Denis Rancourt has, I believe, come up with the most comprehensive analysis of the whole thing. His summary is contained in one of many papers he’s produced, on his own or with others, in the past nine months: All-cause mortality during COVID-19: No plague and a likely signature of mass homicide by government response.
Essentially, he is saying that the vast majority of deaths globally attributed to Covid-19 occurred in care homes between mid-March and mid-May and were caused by psychological stress imposed on old people due to the circumstances created in these homes by lockdown policies.
Professor Denis Rancourt, Ph.D., is a multi-disciplinary scientist from Ontario, who has published more than 100 scientific papers on a variety of subjects, including: physics, chemistry, geology, soil science, environmental science, bio-geochemistry, theoretical physics, alloy physics, magnetism, and planetary science. He has been, since 2014, a researcher with the Ontario Civil Liberties Association, for which he has conducted voluminous research into scientific issues that impact civil rights. Using all-cause mortality — this being the method least susceptible to bias — Rancourt has conducted analyses of data in France, Scandinavia, Canada and the United States, and discovered patterns common to all territories that have not been highlighted by anyone else. His investigations conclusively demonstrate that all-cause mortality in the winter of 2019/2020 was statistically in line with previous years. Covid-19, he found, is not a killer disease, and the attendant ‘pandemic’ has not imposed a death burden in any way out of the ordinary. Many deaths attributed to Covid-19 occurred for other reasons.
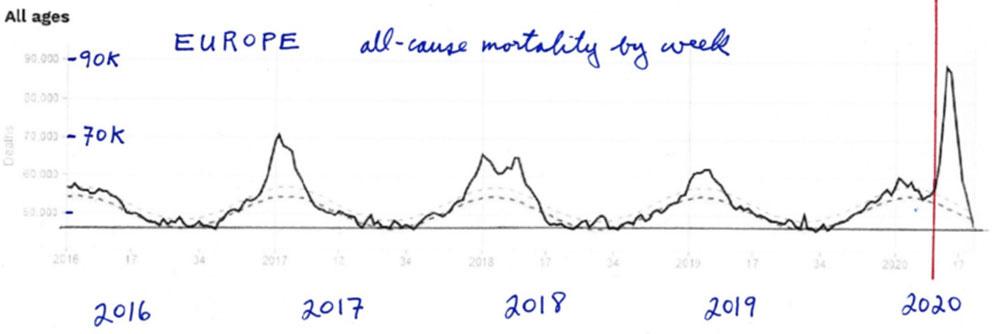
In demonstrating how the trick was pulled off, Rancourt calls attention to what he calls the ‘Covid peak’, which manifested right across the globe — though not everywhere — immediately following the WHO declaration of the pandemic in March 2020. This was a sharp spike in deaths in April, manifesting in numerous countries, and quite unlike any pattern that happens normatively. This spike is present in the data for numerous jurisdictions in Europe and the USA, displaying several unique characteristics: its sharpness, narrowness and remarkable symmetry compared to historical mortality peaks; its lateness in the infectious-season cycle, surging after week 11 of 2020 (mid-March); its uniqueness in recorded history due its large, sharp-peak feature; the synchronicity of its surging across entire continents; and the inconsistency of its manifestation across countries, even between adjoining territories.
Rancourt says it is clear that this repeating artificial spike in deaths arising from deaths caused prematurely due to the systems of care home residents being weakened by panic and stress, with some falling prey to viruses and other infections at the end, is at the core of the meaning of the Covid event.
The data provides the basis for his conclusion that there has been ‘no plague and a likely signature of mass homicide by government response.’
He also says the idea that there was just one virus is ‘a cartoon view of the world.’
He states: ‘These “COVID peak” characteristics, and a review of the epidemiological history, and of relevant knowledge about viral respiratory diseases, lead me to postulate that the “COVID peak” results from an accelerated mass homicide of immune-vulnerable individuals, and individuals made more immune-vulnerable, by government and institutional actions, rather than being an epidemiological signature of a novel virus, irrespective of the degree to which the virus is novel from the perspective of viral speciation.’
These circumstances came to bear primarily in care homes, ensuring that many people locked into these institutions between mid-March and mid-May would die from this particular seasonal virus, SARS-CoV-2, causing the respiratory disease Covid-19, though this was just one among many causes of death, the other being, commonly, co-morbidities that might have in any event caused the deaths of these people over the medium term. The virus itself, he says, is not more virulent than other viruses, and is not ‘deadly’.
The uniquely sharp peak in fatalities, occurring as the flu season was tailing off, simultaneously in many different places across several continents, and directly following the declaration of the pandemic by the WHO, left him in no doubt that ‘there was an acceleration of deaths of vulnerable people due to government responses.’
Many elderly people were essentially locked into nursing homes from about mid-March. The conditions could not have been more suited to creating enormous levels of stress. The patients were locked into institutions devoid of fresh air and sunlight, deprived of the company and affection of their loved ones and, in some cases, even when not subject to Do Not Resuscitate notices, denied medical treatment. They were also, as a result of agreements between politicians and Church leaders, denied the ministrations of priest or chaplains. And every evening, many of them were subjected to the daily death toll delivered by hang-dog Covid tsars via the TV in the corner of their death cells.
And there is an additional factor to be accounted for as a primary consideration: the effects of stress on the human immune system. Bruce Lipton, the American developmental biologist, epigeneticist, stem cell biologist and best-selling author of The Biology of Belief, has elaborated on this point from the broader physiological perspective. In The Biology of Belief, he insisted that stress is responsible for up to 90% of illness, including heart disease, cancer and diabetes. When we are in a constant fear response, our immune systems are compromised because vital resources and energy are being channeled to mobilise a fight-or-flight response. ‘When an individual is in stress,’ he elaborated in a blog commentary, ‘Do Not Fear the Bogeyman’, on the Covid affair, ‘the release of stress hormones (e.g., cortisol) shuts down the immune system to conserve the body’s energy for running away from the perceived stressor, that proverbial “saber-toothed tiger.” Stress hormones are so effective at compromising the immune system that physicians therapeutically provide recipients of organ transplants with stress hormones to prevent their immune system from rejecting the foreign implant.’ Lipton believes that many of the deaths attributed to Covid arose from ‘[t]he media (perhaps in conjunction with the pharmaceutical industry) . . . compromising people’s health using the fear card.’
This is the untold story of 2020: The Year of Merciless Killing.
As fate would have it, this is a topic I wrote about at the very beginning of the Time of Covid, last March. On March 18th, one week after the first Irish death attributed to the SARS-CoV-2 virus, and the day after the then-Taoiseach Leo Varadkar’s televised address to the nation, an article of mine, ‘Covid-19 and the New Death Calculus’, was published by the American magazine First Things. In this article, I picked up on numerous cultural cues I’d been observing concerning the attitudes and policies being demonstrated by official bodies, media people and medical personnel, at the very outset of the ‘pandemic’. (https://www.firstthings.com/web-exclusives/2020/03/covid-19-and-the-new-death-calculus)
Essentially, the article warns against what was about to happen, although I did not at that stage anticipate the cold-blooded calculation that would later emerge as having attended the unprecedented events of that most distressing of springs. I imagined I was seeking to anticipate what I feared might be the inevitable collateral consequences of what I still believed to be a genuine pandemic, albeit in a context of limited medical resources and widespread panic. Professor Rancourt’s analysis addresses the same context but exposes my naivety.
Ireland provides a textbook example of the Covid-peak pattern that Rancourt talks about. On the face of the official data, we experienced one of the highest rates of nursing home fatalities in the world, with more than half of the deaths attributed to the ‘first wave’ of Covid occurring in such homes. This unfolding situation was preceded by a bizarre sequence of events in March that in retrospect takes on a more ominous hue.
On March 6th, Tadhg Daly, CEO of Nursing Homes Ireland (NHI), the umbrella body for Ireland’s 460 private or voluntary nursing homes, announced a ban on what he called ‘non-essential visiting’ to residents in NHI-administered homes. This, clearly, was intended to prevent the virus getting into these homes. The announcement elicited an odd response from the HSE’s Chief Medical Officer, Dr. Tony Holohan, who responded: ‘We ask that no organisation, school or health service provider acts unilaterally. We need to respond to the threat of Covid-19 in unison, following the advice of Public Health.’ Expanding on this decision some weeks later, Holohan explained that his view was that their emphasis ought to be on ‘community transmission’ as there was no way of controlling the spread in ‘any institutional setting’.
Yet, on March 12th, less than a week after Holohan had ordered the reversal of the NHI decision, NPHET issued a directive ordering precisely what Tadhg Daly had sought to implement on March 6th. On the evidence at present available, there is no definitive way of seeing into these events and stating with certainty that this sequence of closing, opening and closing had any specific impact in provoking the extraordinary carnage that was to follow. But it would be at least reasonable to assert that, for six crucial days, just a week after the first recorded case of Covid-19 in Ireland, the virus was allowed to circulate freely in nursing homes, when this might have been avoided. Such an analysis might elaborate that, with the damage done, the homes were closed down for an extended period, with minimum attention paid to the needs of residents, with the results that Professor Rancourt describes as occurring in the general global context.
I am grateful to Colmán Etchingham’s document ‘Coronamania’ for the information that, on May 7th, Dr. Holohan appeared on ‘Today With Seán O’Rourke’ and, reflecting on the events of two months earlier, stated: ‘We’d a number of unilateral actions taking place across society. There was [sic] school closures happening. There was [sic] sporting organisations making decisions. There were other organisations making decisions. And there were certain decisions being made in relation to nursing homes. All of which were not, let’s say, emanating from the public health advice that we were giving. We wanted to have the country move in step with the advice, and have people follow the advice as we issued it. We didn’t want to see a measure like restricting visitation to nursing homes — which is cutting people off from their loved ones —being introduced any earlier.’
‘Any earlier’. This is a strange construction to apply to an initiative that was introduced, cancelled and then reintroduced just six days later. Why were those six days so crucial to NPHET’s and Holohan’s plans? Was it merely a power thing, or did Daly’s jumping the gun cause some other kind of problem? It is as if Dr Holohan was speaking of a plan that was already in place, and was put at risk of disruption by the NHI proposal. It is also noticeable that Holohan sought to clothe the HSE/NPHET countermanding of Daly’s decision in virtue, as though their primary concern was the welfare of residents, whereas we can read from his own construction that they were going to close the homes anyway — just not quite yet.
Colmán Etchingham’s analysis zeroes in on the possibility that the delay in closing the homes may have allowed the virus to find its way into the nursing homes, resulting in the havoc that was to follow. Although I do not believe this is the central issue here, it remains an open question, requiring profound forensic examination.
According to the summary of facts preceding Etchingham’s extensive analysis, Holohan, speaking to Seán O’Rourke, maintained that, ‘because a graph showed a lag of up to three weeks between widespread “clusters” of cases appearing in nursing homes (late March-early April) and the imposition of visiting restrictions, the delay in closing the homes did not cause the numerous numbers of deaths of nursing home residents.’
Etchingham raises questions on this score: ‘Since the spread of the disease, how it is manifested, and the degree to which asymptomatic transmission can occur, are more or less disputed generally, even with regard to old people, this cannot be certain. The argument could be considered a convenient one, excusing Holohan from having to admit the possibility that a mistake was made. . . . The graph allows that Holohan may be right, but it appears that the case is less conclusive than he would have us believe. Whatever about “widespread clusters”, it is noteworthy that the first “clusters” were identified in two separate nursing homes on 16th March, just four days after the revised NPHET advice to halt nursing home visits.’
‘Moreover, if Holohan’s case for self-exoneration in relation to nursing home visits be accepted, it does not seem to have occurred to him (or to O’Rourke, his interviewer) that two further questions are then a logical consequence. If visitors had no demonstrable impact on the spread of Covid-19 in nursing homes, then another cause must be found for the extraordinarily high number of Covid-19 deaths associated with nursing homes (985 or 56% by 14th July). Ireland is at “the upper end of the scale”, compared to other countries, when it comes to nursing home deaths from Covid-19, Dr David Nabarro of the World Health Organisation (WHO) told the Oireachtas Joint Committee in June. If not visitors to nursing homes, what could be the cause of this catastrophic level of mortality, and is it not of the utmost importance to seek answers to that question? Secondly, if admitting visitors to nursing homes had no harmful consequence for infections (and deaths), then why did Holohan and NPHET end visits on 12th March, his qualms about “cutting people off from their loved ones” of six days earlier now discarded without explanation? Not the least shocking consequence of NPHET’s “lockdown” is that so many elderly people died alone, without the comfort of their relatives and friends by their bedsides in their final hours. The inhumanity of this was compounded by the draconian restrictions imposed by the “lockdown” on attendance at and conduct of funerals.’
While endorsing everything Colmán Etchingham says here, and agreeing that these are matters requiring urgent and detailed investigation, I believe that an even more disquieting set of possibilities arises if we apply the Rancourt analysis to the Irish situation. Perhaps here may lie the reason for the ‘catastrophic level of mortality’ in Irish nursing homes. In this analysis, what needs to be focussed on is not the possibility of contagion but the instigation of conditions likely to lead to psychological stress being imposed on elderly people vulnerable to innumerable pre-existing conditions. By this hypothesis, the schmozzle involving Holohan and Daly acquires a different and possibly more ominous significance.
A superficial interpretation of Holohan’s response might be that he simply did not like other actors sticking their oars into his boat space. While the idea of Holohan as control-freak par excellence is far from far-fetched, it does not here seem to provide a total explanation. Why was ‘moving in step’ so important in a situation where Daly appeared to be erring, if at all, on the side of caution, anticipating the NPHET decision by six days? As Etchingham notes, the idea that the health tsars did not wish ‘to see a measure like restricting visitation to nursing homes — which is cutting people off from their loved ones — being introduced any earlier’ does not ring true either, in view of the fact that a few days later they were prepared to countenance precisely that, and leave that situation in place for nearly five months — it being the end of July before NPHET announced that the gradual reintroduction of normal visiting arrangements should begin, and in practice that has yet to happen. (So much for concern about ‘cutting people off from their loves ones’.)
It seems more likely that NPHET’s countermanding of Tadhg Daly’s announcement was based on a realisation that this would amount to a deviation from a fixed plan of which he was unaware: that the NHI closure plan unwittingly threatened some pre-arranged schedule. This realisation may have erupted within NPHET or may have been the consequence of a nudge from elsewhere, perhaps from some agency responsible for monitoring progress towards a narrative crescendo across the ‘common news area’ of Europe and North America. The reversal of that decision, on March 12th, might have been a panicked response to the first announced Irish death from Covid-19 on the previous day, or it may be that, by then, the signal had been received for the roll-out of a plan that was to be played out in numerous locations across the world over the next two months, resulting in the deaths of tens of thousands of elderly people — not from Covid-19, but from the cause Professor Rancourt has adduced: psychological stress imposed by public policy, an outcome that any half-trained epidemiologist might have predicted.
Another matter that surfaced in numerous jurisdictions, including Ireland, was the discharge of people from hospitals into nursing homes, sometimes under governmental edict that such people not be tested on transfer. This occurred in New York, the US state with the highest claimed fatality rates from Covid, as the result of an order by Andrew Cuomo, the Governor of New York state, issued on March 25th. It also became an issue in Ireland towards the end of March, when the HSE, having already directed that only people who had twice tested negative for Covid-19 be admitted back into nursing homes, revised this ruling on March 30th and, along the same lines as Cuomo’s already controversial ruling, removed the requirement for pre-transfer testing and instead advised that those so transferred and exhibiting fever or respiratory symptoms should be isolated in the nursing homes and then tested. The HSE at the time claimed that what it described as a ‘necessary risk’ could be justified on grounds of ‘maintaining access to a critical service’, which Colmán Etchingham plausibly translates as ‘keeping acute hospital services from being clogged up with elderly patients’.
Combining Etchingham's, Rancourt’s and Lipton’s analyses, we can observe the broad context for the necessity that these matters be minutely investigated, most appropriately by a public tribunal of inquiry. The questions to be investigated include: Why did NPHET countermand Tadhg Daly’s announcement of March 6th, and then reverse its own decision six days later?; Why did NPHET on March 30th do away with its own strict preconditions for admitting people back into nursing homes?; How many nursing home residents died ‘of’ Covid rather than ‘with’ Covid?; What, if any, discussion ensued within NPHET about the likely consequences of locking up elderly people in conditions whereby they were likely to become panicked and stressed, and therefore more likely to become ill or suffer an escalation of underlying conditions? Any GP will tell you that an elderly person who has been greatly weakened by heart disease, a stroke or cancer, will frequently contract some form of infection in the final days or hours of life. This can become entangled with the primary cause of expiration, but is rarely deemed a primary cause of death.
From the available evidence, it is clear that virtually all deaths occurring in Irish nursing homes between mid-March and June, and many of those from the beginning of October to the present, have been attributed to Covid-19. Although it is as yet too early to conduct a thorough analysis, it is likely that the accounting of the Winter 2020 death burden attributed to Covid-19 involves many of the same syndromes that characterised the spring manifestation, as well as exhibiting an additional tendency to classify influenza cases as Covid, with the result that, by many accounts, winter flus have all but disappeared.
For several months in the wake of the Irish ‘Covid peak’, the Irish media trumpeted a total figure of 1,776 deaths from Covid — now increased to over 2,000. This was entirely bogus. Successive analyses by both HIQA and the Central Statistics Office reduced this figure to a small fraction by subtracting from the number of people alleged to have died of Covid those who had merely died with Covid — the reliability of diagnosis being in many cases suspect because of the unreliability of the PCR test and inconsistencies in the methodologies applied in certifying such deaths. At one point, around the end of the summer, while the media were still giving the 1,776 figure (and counting enthusiastically) a CSO calculation put the figure of deaths from uncomplicated Covid at 76. This is in line with figures recently published for the United States by the Center for Disease Control (CDC), which reveal that only 6% of all deaths labelled as Covid deaths were solely related to the virus SARS-CoV-2. The remaining deaths had at least one, and more often two or three co-morbidities.
Moreover, we know from the UK that, as early as the end of the summer of 2020, approximately 40% of the deaths that had been attributed to Covid-19 had in fact been the result of lockdown policies impinging on other aspects of the health services: people missing cancer checks, delays going to Emergency in the event of suspected heart attacks, strokes, and so forth. As time moves on, the numbers of such cases are likely to increase.
In my First Things article in March, linked above, I wrote:
‘Now, in the first rush of the coronavirus crisis, I sense that the phrase “a good innings” has taken on an ominous ring. Its logic has begun to be applied not to the dead but to the still living. You hear it all the time: Those who die will be the old. It is not matter-of-fact observation, but a kind of death sentence. It is preparing us for something: the next phase. . . . My sense has been that our culture is already desensitizing us for this next phase by “training” us to see illness as a kind of luxury, treatment as a concession, and the old as a separate category of the human. Because the old are increasingly hidden away from everyday society in purpose-built nursing homes, when we happen upon the old we are already beginning to look away from their frailty, and therefore their, and our own, humanity.’
In part, I believe, this is the central mechanism of the Covid operation: engineered deaths of the elderly to bump up the fatalities and scare the wider populations. If this seems preposterous, then I ask you, in the Irish context, to contemplate the piece of legislation that, aside from Covid pseudo-law, took up most Oireachtas time during the middle months of 2020: the Gino Kenny/People Before Profit ‘Dying with Dignity Bill 2020’.
Imagine: the country had not even begun to emerge from the trauma of observing a thousand of its elderly citizens wiped out, ostensibly by a ‘deadly disease’, but more likely, as we have seen, by induced psychological stress resulting from government policy and media-generated panic. And the first thing on the agenda was to introduce measures which in the future would allow the same kind of thing to be achieved without any kind of subterfuge at all.
In October, a government-sponsored amendment ostensibly calculated to delay a vote on the Second Stage of the 'Dying with Dignity Bill 2020' was defeated in Dáil Éireann by 86 votes to 65. This was remarkable in view of the fact that, between them, the three government parties commanded 84 votes out of the 160, which at the least suggested a lack of enthusiasm within for the government’s own implied policy of dissatisfaction with the Bill. The Second Stage of Kenny's Bill was then put to a vote, and was carried by 81 votes to 71, signalling that 152 voted, again with two abstentions, with 6 absent from the Dáil Chamber for that vote.
This tells us two significant things. One is that, despite seven months of pretending that they were interested in ‘saving lives at all costs’, more than half the members of the main parliamentary forum were in favour of creating conditions whereby old people might be induced to agree to accept death by medical intervention, thinly disguised as ‘choice’. The second thing it tells us is that the government wishes to effect this radical change in Irish culture without itself having to carry the can for it, and is using proxies to achieve its aims in an underhand fashion.
A radio debate a month earlier between the nominal proponent of the Bill, Gino Kenny, and David Quinn of the Iona Institute demonstrated that Kenny had not the faintest idea what was in his Bill, or what was not in it. In a series of almost comical exchanges in a Newstalk debate, Quinn read out sections of the Bill which contradicted statements just made by its supposed architect. According to a report by Niamh Ní Bhriain on gript.ie, Kenny said that his bill sought to help those who had a condition that was ‘progressive, unbearable and painful’ and who, when they were ‘coming to the end of their life should have a choice to end their life.’ Quinn pointed out that, despite Kenny’s claim, no reference was made in the Bill to unbearable pain. ‘Gino used words like painful and unbearable but I can’t find them in his Bill,’ he said.
Kenny asserted: ‘It says in the legislation that, you know, somebody is coming to the end of their life, there’s a very very short period of time, when they come to their terminal illness, and that person is conversant to make that decision.’
Quinn asked, ‘Where does it say that?’
Kenny replied, ‘No, It does, it does’, but he was unable to point to where it said it.
This indicated that either Kenny had suddenly been struck down by a degenerative brain disorder or someone else was the architect of this Bill, designed to change the ethical ecology of Irish life for all time.
And Ireland is not alone in this odd juxtapositioning of contradictory categories of ‘compassion’: another formerly Catholic country, Spain, is currently taking final steps towards a similar end. On Thursday December 17th, Spain’s Congress of Deputies, the lower house of the national parliament, voted in favour of legalising euthanasia by a vote of 198-138. The legislation next moves to the upper house, the Senate, where it is expected to pass. And this at the end of a year in which Spain had experienced — or so we were led to believe — one of the highest Covid fatality rates in Europe. Interesting — no?
In both countries, of course, it is leftists who push these agendas, while posturing publicly as defenders of the old and vulnerable. During the spring and summer of 2020, while the relatives of the prematurely despatched elderly were burying their loved ones in the fashion of convicted murders in the corners of prison yards (minus only the quicklime), People Before Profit goons were to be found on the streets of Dublin leading assaults on those questioning the lockdown. And, since said lockdown was emerging as the context of the most horrific mass homicide in recent memory, it will come as no surprise to any sentient being that the party, under instructions from quarters that can only too readily be guessed at, was at the same time busily helping to clear the way for the legalised destruction of countless lives into the indefinite future.
Of course, the practice of expediting death deemed inevitable has become normalised in Irish hospitals and otherwise. Morphine is the most commonplace method in use for this purpose, and is administered by many GPs under the guise of relieving pain and distress, often without consultation with the family of the person being despatched.
These practices are, on the one hand, camouflaged by euphemism and hair-splitting, and at the same time deemed to be ineluctable ‘compassionate’ aspects of life and death in a ‘post-Christian’ society. As with many aspects of our lives, both public and private, these have been subject to acceleration in the Time of Covid.
There is nothing compassionate in any of it. Such practices take us backwards, not forward. In primitive human societies, human sacrifices to the gods were regarded as a guarantor of continuing prosperity and protection. Human mythology is studded with stories of human sacrifices of first-borns, of widows burned alive on the graves of their husbands, of willing victims giving their lives so that their decomposing bodies might give life to plants by which their communities could continue to live. Symbolically, then, the events surrounding the Easter of 2020, and some of the rhetoric which preceded them, take us back towards such a culture of barbarism rather than forward to some Promised Land of empathy and compassion. We were told we were (mandatorily) sacrificing a little freedom to prolong the lives of the old. On the contrary, the old were sacrificed anyway, so that the young might be reduced to the walking dead.
Your last, chilling, sentence sums the whole thing up: '...the old were sacrificed anyway, so that the young might be reduced to the walking dead.' What can ordinary people like me do? Am storming heaven. What else?