Lockdown stops the hearts of free peoples
Lockdown as a ‘remedy’ for Covid remains unquestionable despite scientific studies showing it as ineffectual and dangerous. Yet, those who extol ‘the science’ make this issue an exception.

Before 2020, the term lockdown had one meaning for most people, this concerning the life of prisons. Before that was an archaic meaning related to timber transportation — a ‘lock-down’ was a piece of wood for securing pieces of timber together when they were being carried by river on a raft. Apparently, from about the 1970s, the word came to mean exclusively ‘the confinement of prisoners to their cells for all or most of the day as a temporary security measure’ (for example, after a riot by prisoners). It is a tribute to the ubiquitous nature of the propaganda we have witnessed in the Time of Covid that already the altered meanings arising from the ‘pandemic’ of 2020 have been uploaded to online dictionaries. Now, according to the Merriam Webster dictionary (since 1828), ‘lockdown’ means this also: ‘A temporary condition imposed by governmental authorities (as during the outbreak of an epidemic disease) in which people are required to stay in their homes and refrain from or limit activities outside the home involving public contact (such as dining out or attending large gatherings).’ The Merriam Webster dictionary adds the following clarifier: ‘NOTE: Individuals who are employed in various occupational fields (such as healthcare, public works, law enforcement, and food supply) considered essential to public health and safety may continue working outside the home during a lockdown.’
This normalisation of the word in its new incarnation is matched by the behaviour of people in the non-etymological world. If, as you walk about, you listen attentively for snatches of the conversations of passers-by, you will catch it on the breeze in constructions like ‘before the lockdown’, ‘since the lockdown started’ or ‘in the first lockdown’, used in a manner remarkably devoid of rancour. The tone is always matter-of-fact, bearing none of the connotations of the word that persisted until this time last year. In these new uses it is nearly always clear that the condition it refers to is itself benign, albeit sometimes demanding or irksome. The tone is as though in reference to a kindly if stern mother-in-law, or perhaps an austere but occasionally somewhat benevolent headmaster. Or perhaps reminiscent of the way Catholics might still occasionally refer to ‘the Lent’ as though to some severe taskmaster who nevertheless is only out for their good.
Implicit in all this appears to be a watertight assumption that lockdown is necessary and even good, and this would seem to embrace the idea that it is, in some sense, however woolly or vague, a ‘remedy’ for Covid.
There is a strange lacuna, however, in virtually all casual discussion of the merits of the ‘pandemic’: the question as to whether there is any necessity for lockdown in any circumstances whatever, still less the present ones.
Of course, the proportionality of the lockdown is always by definition central to all such discussion, but what is interesting is that almost all of them immediately short-circuit into assertions relating to the relative gravity of the specific ‘novel coronavirus’, as though establishing a single point of Covid’s enhanced powers to sicken would be enough to justify any measure taken in the name of containing it. People focus on the nature or severity of Covid, usually as relayed to them by ‘experts’ via the media. Such conversations tend rapidly to break into declarations like, ‘It’s not the flu — it’s much worse than the flu!’, or ‘Well, I wouldn’t like to get it!’, as though these represented definitive and closing commentaries not merely on the gravity of the condition but also on the validity of any conceivable remedy, including lockdown. It is almost as if people use ‘lockdown’ as a synonym for ‘Lemsip’ or ‘Lucozade’, though, to the ears of the sceptic, hearing it erupt in casual conversation along the street it is a little like passing a huddled group of Death Row prisoners and hearing a heart-stopping, throwaway ‘potassium chloride’. The comparison is not too strong, because lockdown just as surely stops the hearts of free peoples.
There is a quirky equation to be attempted here involving quantities like ‘progress’, ‘freedom’, ‘democracy’, and ‘comfort’. Mass lockdowns would have been impossible even at the end of the last century: most people would have revolted, for the very good reason that there were few alternatives to going out and doing a day’s work to put bread on the table. There were no takeaway deliveries, no WI-Fi for home-working, no Netflix to substitute for the thrills of the Great Outdoors.
There are many conundrums here that we’re only beginning to scratch the surface of: Why are we not protesting at this restriction of our freedoms, for a ‘pandemic’ involving a virus with a 99.98 per cent recovery rate for people under retirement age, that is largely fatal only for the very elderly and frail? What was so wrong about the ‘old normal’ that makes us thrilled to stay at home for a year and counting, waiting to be told how we shall live our lives in the future? Why is Ireland apparently content to have the most restrictive lockdown in Europe? What has happened to the fabled nous of the Irish, the cuteness that once allowed Paddy to mind mice at crossroads while peeling an orange in his pocket?
Lockdown is a non sequitur to just about anything. The only thing we need a lockdown from is the kind of moron politicians who have steered us into this disaster, with their mixture of piety, stupidity, mendacity and arrogance. The only pandemic that exists is a pandemic of lying. Here be a question: What are they going to do to us if there ever is a real pandemic, like in the movies, with healthy young people falling dead in the street, and ambulances crashing into hearses in their rush to flatten the bodycount curve. Is there anything beyond lockdown other than the kinds of things we are not permitted to compare the Time of Covid to?
Or would we even need to be locked down if there was actual danger? Obviously not. The point of lockdown is itself: It is a weapon of mass coercion and humiliation. As Thomas Sheridan so pertinently asks: Where is the love? That’s it: They have stolen the love — from the dying pensioners who have spent their lives caring for others whom now they are not permitted to bid goodbye; from the teenage would-be lovebirds who are denied the sacred mystery of the birds and the bees; from the children who cannot see their parents’ smiles though their ‘face coverings’. And on, and on.
Some residue of the prison-related meaning of ‘lockdown’ therefore remains and is intended to. This leftover life of the prior meaning has two intertwined elements: the idea that it relates to prisoners, and the idea that these prisoners have done something wrong and so deserve to be punished. These meanings, too, can be picked up on the breeze, a certain masochistic sheepishness betraying a wry awareness of some undeclared, unfocused guilt or culpability. And, when you think about it, that’s actually it: The reason people have mostly not seemed to resent the lockdown is that they haven’t: They believe it’s no better nor worse than they deserve. Perhaps all their lives they have longed for a bunch of thugs in shiny suits to come along and treat them like dirt. Perhaps this is the real pandemic: a pandemic of masochism, of mandatory perversion — the perversion of subs and doms rendered political and total, as in totalitarian. Perhaps this is the scariest aspect: that too much comfort and freedom have left many of our seemingly butter-wouldn’t-melt neighbours longing for a bit of rough. And the art of the politician in the third millennium is the capacity to be able to see such things coming.

The graphs above and below, produced for me by Des O’Keefe, refer to the first lockdown in Ireland, in March/April 2020, and seek to demonstrate that this could have had little if any effect on curtailing deaths from Covid-19. They operate off a simple formula and the method can be replicated and applied to any situation or jurisdiction. The graph above shows, in as far as possible, the pattern of deaths that occurred between mid-March and early May. The second graph combines this pattern with that of ‘reported deaths’, which is to say deaths at they were reported, a process that became mysteriously subject to increasing irregularity in the final week of April. The vertical lines indicate various stages of the lockdown, from the closure of schools on March 12th to in effect a generalised house arrest on April 7th.
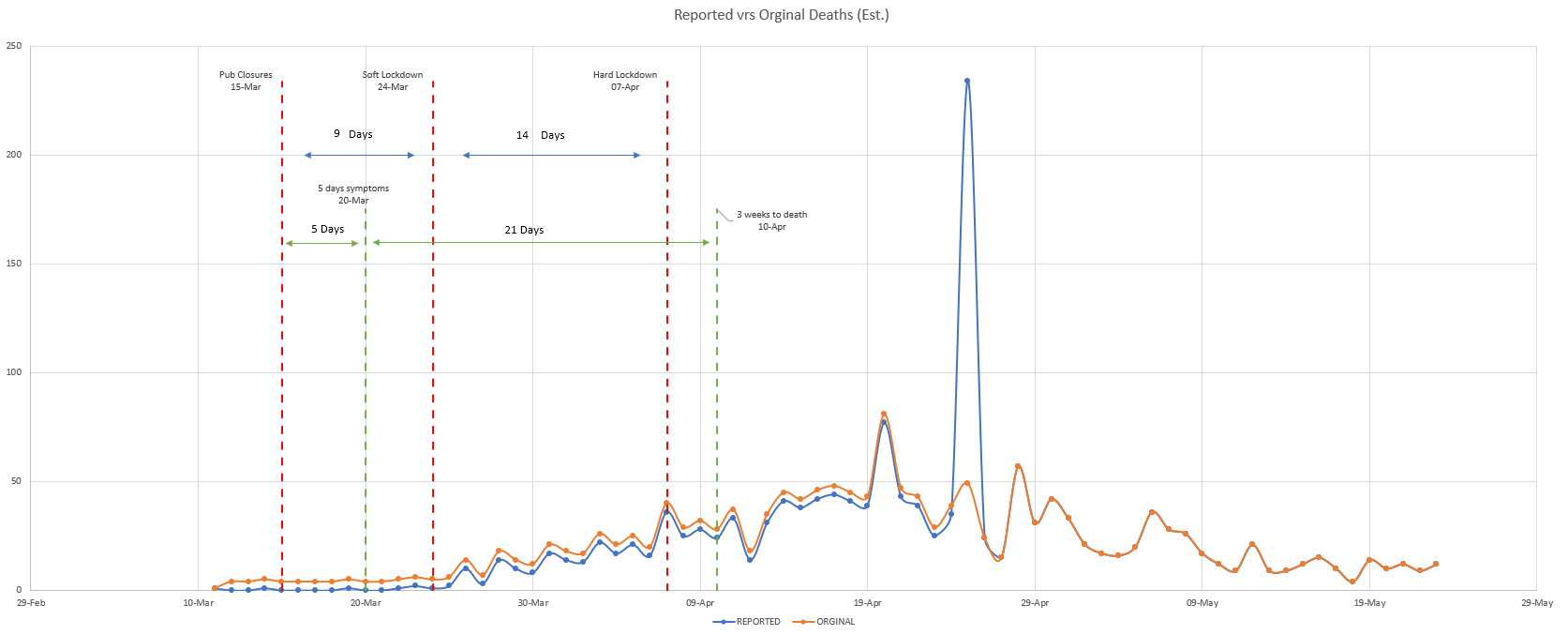
The graphs allow one to measure the likely impact of various stages of the lockdown process, from ‘soft’ (without state coercion) in mid-March to full-on Garda enforced regulations in various stages from April 7th.
Three to four weeks is taken as the standard or average time between emergence of symptoms of Covid-19 and death where this occurs. This makes clear that — at the very best, taking a conservative average of three weeks from infection to death — only those measures taken during March could have had any effect. Therefore, since the peak of fatalities occurs in or around April 20th, and the rate of deaths decreases fairly dramatically within days afterwards, only measures applied — at the latest — before March 31st could circumstantially be hypothesised as having had any effect on the sudden and dramatic decrease in fatalities. In addition, and for different reasons, there are reasons for disputing whether measures introduced in mid-March could have had any material effect on subsequent mortality patterns either.
‘Lockdown’ Irish-style entailed, firstly, closure of all educational institutions and childcare facilities, museums, galleries and tourism sites — all from 12th March. These were effected by Statutory Instruments issued by the Minister for Health following recommendations by NPHET, the health junta. Restriction of visiting at nursing homes, among other institutions, was also ‘recommended’ at this point. Closure of pubs took effect from Sunday 15th. A NPHET recommendation of March 24th advocated the closure of ‘non-essential’ shops, and the limiting of cafes and restaurants to takeaway service. NPHET also ‘recommended’ that sport and a plethora of other activities and occasions of public gatherings be shut down, and that people work from home if possible, and this was immediately translated into a Statutory Instrument. A letter issued by the Chief Medical Officer, Tony Holohan, on 27th March, announced that ‘NPHET agreed to recommend’ an end to all ‘non-essential’ travel more than two kilometres from home and that ‘cocooning will be introduced for those over 70 years of age’. This, in effect, full-scale ‘hard lockdown’ was complete and unleashed by 7th April, when Tony Holohan’s letter of that date announced that ‘NPHET considered that the powers contained in the draft Regulations under the Health (Preservation and Protection and other Emergency Measures in the Public Interest) Act 2020 should be available for use by the Gardai in the coming weeks’. Operation ‘Fanacht’ — the Irish for ‘remain’ — was underway.
As already stated, we can observe two apparently contradictory phenomena from the graphs above. The first is that there is an absence of symmetry between the earliest lockdowns from March 12th onwards and the spike in mortality (original deaths graph) that peaked on April 20th. Had these measures been effective, where is the evidence to demonstrate it? The April 20th spike of deaths implies a pattern of infections beginning sometime around or shortly after March 24th. For the measures introduced in mid-March to be deemed in any sense effective, we should see a sharp decline in deaths sometime in the fist ten days of April. Instead, we see an almost relentless climb in this period, the decline occurring almost three weeks later.
The spike in deaths on April 20th, then, occurs both too late for the measures introduced in mid-March and too early for any measures applied after April 1st to have had any function in provoking these patterns of mortality. The sudden fall-off in deaths from about April 20th — confused somewhat by the delayed reporting of many deaths, but still undeniable — would have arisen from a fall-off in infection approximately occurring in the last week of March — which is to say that, of all the measures, only the shop closures from March 24th might have had any input, and this proposition is rendered dubious by the fact that most of the deaths were occurring in care homes. At a minimum, it can be conclusively stated that measures introduced on April 7th, which in effect imprisoned people in their homes and prevented them travelling beyond 2km thence, were entirely irrelevant to the fall-off in deaths in late April, and had no significant role in ‘flattening the curve’.
N.B. The distinction made in the graph between ‘reported deaths’ and ‘original deaths’ is an attempt to (somewhat speculatively) correct for the fact that, towards the end of the cycle, on April 25th, the authorities published an amount of deaths that had occurred some (indefinite) time beforehand. A simple graph depicting ‘reported’ deaths would therefore have distorted the picture. The ‘original deaths’ (estimated) are an attempt to spread these fatalities over the period in such a manner as to more or less contextualise them correctly. But, even with this adjustment, there appears to be an unexplained dip around April 27th or, alternatively, a likewise unexplained secondary spike on April 28th, either or both of which interrupt an otherwise unbroken downward trend. The graphs may therefore not reflect the actual mortality patterns with perfect accuracy, but they certainly provide an approximately correct picture and are an improvement on the alternative. [It is unclear whether this late reporting of some deaths was a mere clerical failure or something more ominous. Certainly, someone unaware of the delay in reporting some deaths, and their being allowed to accumulate before being released on a single day, April 25th, might be misled into thinking that the peak of deaths occurred nearer the end of April than it did. This might well indicate an attempt to retard the pattern of mortality to make it appear to tie more closely with the introduction of the hard lockdown in the early days of April, thus ‘proving’ its efficacy, but this cannot be averred with certainty.]
All this reveals that, if anything at all of the measures introduced by the authorities might be said to have had an impact in reducing fatalities, it was the ‘soft’ measures like social distancing that had been running from late March, and just possibly the closure of ‘non-essential’ shops, restaurants and cafés from March 24th.
Although Ireland and other Western societies have in the past experienced innumerable pandemics — most notably the ‘Spanish Flu’ of 1918 — it was never before proposed that the locking down of societies, the closure of businesses, workplaces and schools, and the partial imprisonment of whole populations in their homes and localities, might offer any kind of remedy for the threat arising. While, in the course of the 1918 episode — the worst in recent history — certain activities were subject to restriction for a limited period of time, there is no record of any imposition of a population lockdown in response to that disease.
No scientist had ever publicly supported imposing lockdowns until Xi Jinping, General Secretary of the Chinese Communist Party (CCP), personally authorised the unprecedented lockdown of Wuhan and other Chinese cities beginning on Jan. 23rd, 2020.
The World Health Organisation’s 2019 guidance for pandemic influenza, Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza, did not advise border closures, mass contact tracing, or quarantine even of ‘exposed individuals’ under any circumstances.
When the lockdown of Hubei province began, the WHO’s representative in China, Gauden Galea, told the Associated Press. ‘To my knowledge, trying to contain a city of 11 million people is new to science. It has not been tried before as a public health measure, so we cannot at this stage say it will or will not work.’ UK newspaper, The Guardian, which has since become a key media cheerleader for lockdown, editorialised: ‘That the Chinese government can lock millions of people into cities with almost no advance notice should not be considered anything other than terrifying.’ The editorial continued: ‘International law is clear that during a time of public health emergency, any restrictions on human rights should be based on legality, necessity, proportionality and grounded in evidence. The international community should support all efforts to end this outbreak, but human rights should not be a casualty to the coronavirus crisis.’
These expressions of concern did not deter the WHO from, just days into the Chinese lockdown, effusively praising the Chinese Communist Party’s ‘unprecedented’ response: ‘The measures China has taken are good not only for that country but also for the rest of the world,’ a WHO statement declared, producing not a shred of evidence for this contention. WHO Director Tedros Adhanom praised China for ‘setting a new standard for outbreak response.’ Shortly thereafter, the WHO held a press conference during which Assistant Director-General Bruce Aylward told the press: ‘What China has demonstrated is [that] you have to do this. If you do it, you can save lives and prevent thousands of cases of what is a very difficult disease.’ Two days later, in an interview for China Central Television (CCTV), Aylward instructed the world: ‘Copy China’s response to COVID-19.’ Yet no analysis was forthcoming by way of demonstrating a connection between the lockdown policy and any change in the patterns of spread, infection or fatalities in China.
It appears that, under pressure from the WHO, the imposition of lockdowns in Wuhan and other areas of China — a nation unconstrained by concern for civil liberties and constitutional norms — started a domino effect whereby, from late February 2020, one country after another imposed the same draconian and hitherto untried measures on their citizens. With minimal analysis, study, assessment or review, or without consideration of their likely collateral effects on healthy people or functioning societies, these measures were summarily adopted and applied by democratic governments all over the world.
Certainly there is no evidence whatsoever of such measures ever having been tried and proven in Ireland or in any other Western European country, or in the United States. Not only were lockdowns historically unprecedented by way of response to any previous epidemic or pandemic, but they had not been given so much as a mention in recent guidance offered by the US Center for Disease Control and Prevention (CDC). In the event of highly infectious influenzas, the CDC guidelines provided only for ‘voluntary home isolation of ill persons,’ and the additional ‘recommendation’ of ‘voluntary home quarantine of exposed household members in areas where novel influenza circulates.
In February 2020, a team from Imperial College London led by physicist Neil Ferguson ran a computer model that was to play a grotesquely disproportionate role in the justification of lockdowns by many governments. Imperial College forecast a number of potential outcomes, including that, by October 2020, more than 500,000 people in Great Britain and 2.2 million people in the US would die as a result of Covid-19, recommending months of strict social distancing measures to prevent this outcome. From these projections a figure of 85,000 deaths was extrapolated by the Irish Government by way of estimating the likely consequences of allowing the virus to run its course here. These projections were subsequently revealed as dramatically overstated. Thus, we observe that a prestigious institution producing particularly alarmist models can have a distorted impact on political discourse. In this case, the institution in question not only consistently and egregiously erred in grossly exaggerating the risks of mortality, but itself became an active agent in promoting the unprecedented lockdown policy.
On March 24th 2020, just four days after the new Covid laws had been rammed through the Oireachtas, the then Taoiseach Leo Varadkar insisted that the country was ‘not in a lockdown’. He said Gardaí would encourage groups to ‘disperse’ on the streets and ‘move on’ so as to avoid ‘overcrowding’. ‘I wouldn’t use the term lockdown, and that’s for very good reasons,’ he said. ‘I’ve come to learn over the past week or two that lockdown seems to mean very different things to different people, and in different countries, and therefore can cause confusion, and we need clarity, rather than confusion.’
The UK situation, he said, because ‘people can still go to work, go to the shops, the bank, the post office, even B&Q or the pet food store, go for a run, meet with another person outside’, was ‘not a total lockdown’.
‘And I had heard that Italy was in a total lockdown and yet I found out a few days ago that there were still factories and construction sites open. So I think it’s a term that actually causes more confusion than clarity and therefore is one that I wouldn’t use and don’t intend to use in future.’
Varadkar, like other Irish politicians, became increasingly at ease with both the word ‘lockdown’ and the associated concept. The measures introduced by the Irish Government under cover of the ‘Health (Preservation and Protection and other Emergency Measures in the Public Interest) Act 2020’ and the ‘Emergency Measures in the Public Interest (Covid-19) Act 2020’, although presented to the public as a tried-and-tested remedy to the alleged threat to the public represented by the virus SARS-CoV-2 virus, and the allegedly resulting condition named as Covid-19, had never before been implemented anywhere in the world in any analogous or comparable situation. Over the past year, they have subjected formerly free peoples to intrusion, threats, arrest and actual state violence, in a manner not seen in our societies for a century or, in many cases, much more.
People who depend on legacy media for understanding any aspect of the Covid narrative are by definition utterly misled. This deception applies in particular to the effects of lockdown. Such people will have been led to believe — not by factual or explicatory demonstration, but by innuendo, hectoring and bluff — that lockdowns are ipso facto a remedy to the spread of infectious diseases. Not only is there no evidence of this, but the evidence gathered thus far is directly to the contrary.
Sweden, the most examined example of a country that refused to lock down its population, has been subjected to much legacy media disinformation campaigning. Sweden notably confined its response to closing schools and colleges for older children, declined to mandate face coverings and kept its pubs and restaurants open. There have been attempts to suggest that mortality from Covid in Sweden has been out of kilter with the rest of Scandinavia and Europe, but these analyses tend to distort the general picture and the specifics of Swedish demographics. Far from having among the worst Covid mortality rates in Europe, Sweden is about the middle of the table, currently at about 128 deaths per 100k population, compared to figures of 204 in Czechia, Belgium with 195, and 187 in the UK. The Swedish mortality rate has consistently fallen about halfway between Ireland’s and those of the UK, Italy and Spain. And this is purely on raw figures, which conceal a dramatic factor concerning Swedish demographics. In the comparison with Ireland, for example, Sweden has per capita approximately 50 per cent more people over 65 — the most vulnerable categories in the context of respiratory diseases — and the Irish and Swedish mortality rate have reflected this divergence more or less precisely and consistently over the past year, a factor rarely alluded to in self-congratulatory Irish analyses. The broad pattern between Ireland and Sweden over the past year, adjusted for the demographic disparity, is extraordinarily similar given how different have been the overall policy responses between the two countries. And, when you then factor in that Sweden has managed to avoid the many destructive aspects of lockdown, it becomes clear that its chosen course was by far the more rational and all-round effective.
On that question also, Norway, which shares a border with Sweden and was one of the countries with which Sweden was unfavourably compared, created shock waves last summer when it repudiated its own hard lockdown policy. In late May, the Norwegian Public Health Authority (NIPH) issued a report admitting that the virus was already on the wane at the time the lockdown was ordered. In early June, Norway’s prime minister Erna Solberg, said in a television interview that her government’s approach had been over-cautious, ‘misguided’ and largely based on unwarranted fears. Under pressure of the international consensus, Ms Solberg admitted, ‘worst case scenarios became controlling.’
In the United States, in September 2020, a survey by analytics firm TrendMacro tallied the cumulative number of reported Covid-19 cases in each state as a percentage of population, based on data from state and local health departments aggregated by the Covid Tracking Project. The survey found that locking down the economy didn’t contain the spread of Covid, and nor did reopening in summer unleash a second wave of infections. The survey then compared these results with the timing and intensity of lockdowns in each state, measured not on the basis of government mandates but by observing with the aid of anonymised mobile phone tracking data what people in each jurisdiction actually did, compared to their baseline behaviour before the lockdowns. The survey found a strong correlation between lockdown and spread of the virus, and heaviest caseloads in states like New York, Michigan, New Jersey and Massachusetts, which had the harshest lockdowns. In measuring the effects of reopening, TrendMacro used the same methodology and found a ‘weak’ tendency for states that opened up first to have the lightest caseloads, but also detected no correlation between opening up and outbreaks of a ‘second wave’ in states like Arizona, California and Texas.
Presenting the research in the Wall Street Journal, Donald Luskin, chief investment officer of TrendMacro, observed:
‘The lesson isn’t that lockdowns made the spread worse — though raw evidence may suggest that — but that lockdowns probably didn’t help, and opening up didn’t hurt. It defies common sense. In theory, quarantine ought to control the spread of an infectious disease. Evidently not in practice, though we are aware of no researcher who understands why not.’
‘[T]here is no escaping the evidence that, at minimum, heavy lockdowns were no more effective than light ones, and that opening up a lot was no more harmful than opening up a little. So where is the science that would justify the heavy lockdowns many officials are still demanding?
A similar pattern was identified in a survey of countries detailed in a July article in The Lancet, which concluded that ‘A longer time prior to implementation of any lockdown was associated with a lower number of detected cases.’
A study conducted in Stanford University California, during 2020, and published in January 2021, concluded that mandatory stay-at-home orders and business closures had no significant beneficial effect on Covid-19 case growth and may have exacerbated the spread of infections in nursing homes. This survey used data collected in the spring of 2020 which compared outcomes in Sweden and South Korea, neither of which had introduced harsh lockdowns, with the UK, France, Spain, Germany, Italy, Sweden, the US and Iran, all of which had introduced ‘full-blown’ lockdowns. This survey found ‘no clear, significant beneficial effect’ of lockdown on the number of cases in any of the countries surveyed. It also found that restrictive ‘non-pharmaceutical interventions’ short of lockdown — such as reduced working hours, working from home and social distancing —helped curb the rise of infections in nine out of 10 study countries, except for Spain, where the effect was ‘non-significant.’
The research went on to suggest that empirical data from the waves of infections later in 2020 show that restrictive measures failed to protect those most vulnerable to infection. It found that the levels of fatalities occurring in care homes, among the categories of people most vulnerable to respiratory infections, was often higher than in the wider population in areas where lockdown was most severe.
Reflecting on the comment by Donald Luskin of TrendMacro, that some of the findings of their survey ‘defy common sense’ — in particular that the virus appeared to spread more quickly in harsh lockdown environments — reminds us that we need to move away from theories about lockdown that automatically credit the measure with capacities that have never been ascribed to it by actual evidence. Similarly, in a note on the Standford study, the researchers described as ‘counterintuitive’ their own finding that regions with the harshest lockdowns also had the highest rates of care home mortality. For those familiar with the research of Canadian scientist Denis Rancourt, however, there is nothing counterintuitive or non-commonsensical about any of this. As outlined in my end-of-2020 article The Year of Merciless Killing, Rancourt postulates that the sharp, narrow Covid mortality spikes experienced in many jurisdictions last April arose not from infection but from stress imposed by lockdown measures and the atmosphere of panic imposed by government policies and media scaremongering. Thousands of elderly people were essentially locked into nursing homes from about mid-March in conditions bound to provoke enormous levels of psychological stress — stress being an accelerant on the kinds of respiratory condition commonly afflicting the aged. Many people died as a direct result.
This is just one promising area of exploration as to why lockdowns appear to be having the precisely opposite effects to those claimed on their behalf. Another is that whereas, in the general context, lockdown measures may well be suppressing the virus in accordance with normative intuition, they may also be facilitating a culture of survival-of-the-fittest in the context of mutations of Covid, eliminating the lesser strains but leaving untouched the more virulent and transmissible, which lie in wait and strike in moments of unwariness. Being stronger, these variants are coming to dominate the Covid Olympics and are becoming increasingly impervious to the kinds of measures — face coverings, social distancing, stay-home-save-lives — that we assume must work because, well, they must. On the contrary, precisely these measures may be what are causing the virus to mutate. It seems ‘obvious’ that separating people and forbidding them to mingle must have a positive effect. But the science says otherwise and here, uniquely under Covid-related headings, authorities chose to turn a blind eye to what the science is saying.
Assumptions tend to make for good scientific starting points but rather bad conclusions, especially in the teeth of the facts. Far worse is that, in order to fudge the incompatibility between theories and outcomes, the authorities, on a practically universal basis, have embarked on a campaign, with the aid of bought journaliars and ego-driven scientists, to manipulate and falsify the data or, more often, simply ignore the evidence so as to continue pursuing their decrepit hypotheses.
The criminal aspects of this reside in how madly disproportionate the lockdown measure manifestly is. Although Ireland has so far carefully avoided any investigation of the baneful effects of lockdown, these will undoubtedly emerge in due course. Other countries are already building pictures of this dark side of their own lockdown enthusiasm.
In the UK, an Office of National Statistics (ONS) analysis of deaths there between March and September 2020 found 24,387 more deaths-at-home than normal in England, and 1,644 in Wales. This equated to an extra 100 people dying at home every day — 400 daily deaths as opposed to a normal attrition of 300 — mostly unrelated to Covid. The ONS analysis confirmed that, even after the peak of the epidemic, the attrition rate remained at around 400 a day and showed no sign of declining. The very strong indications are that most of these were lockdown-related deaths. The ONS found that, in England between March and September, an extra 1,705 men had died from heart disease at home — 25 per cent more than normal. In Wales there was a similar rise (22.7 per cent). Deaths from dementia and Alzheimer's disease at home in the same period increased most among women — with 1,400 more than normal. While deaths from such conditions also rose in care homes, hospital deaths from dementia went down — by 40 per cent in England, and 25 per cent in Wales. Overall, the spike in excess deaths was attributed to a combination of people being too frightened to go into hospital and disruption of services.
On October 19th, 2020, the day the second Irish lockdown was announced, the UK Daily Mail reported that 50,000 children had surgery postponed in the UK in 2020, while treatments for strokes had fallen by almost 50 per cent. In just one month of the UK lockdown, one in five people was found to be suffering from depression. The Mail, which based its report on information gleaned in an audit of 132 studies from journals, academics and charities, put the total number of excess deaths at home of people who normally would have been treated in hospital at 25,000. This was at a time when the death toll claimed for Covid-19 was 43,700, suggesting that some 35 per cent of all excess deaths were due to the lockdown. The Mail also reported a huge backlog in NHS treatment estimated as likely to cause a 20 per cent rise in cancer patient deaths. Organ transplant operations had fallen by two -thirds while waiting list deaths in this category had doubled.
Since more than half of deaths in the UK — as in Ireland — had occurred in care homes, these figures suggested that between 10 and 20 per cent of excess deaths, but no more, might definitively be attributed to Covid. Applying these metrics to Ireland would appear to reduce the estimated Covid death toll to something in the region of 200 Covid deaths over the first six months of the ‘pandemic’, rather then the approximately 2,000 deaths claimed for that period by the authorities. The situation should become somewhat clearer with the publication of final excess mortality rates for 2020, which will be concluded and published next month.
The idea of a lockdown as a solution to a virus is a little like a sledgehammer used to swat flies: it promises to create far more problems than it solves. Even at the basic level of human immunity, the idea of stopping a virus in its tracks would, if it were not outright impossible, be counter-productive. It is one of the many paradoxes of the human condition that we stay well by regularly becoming infected with things that make us unwell. That’s how our immune systems strengthen and remain efficient. As our grandmothers told us, we have to eat a bucket of dirt before we die.
Another, related paradox is that rest and recuperation help us recover from illness, but at a certain point we require to get up and outdoors so that the process of recovery can continue. That’s because the human body loses function and cohesion much more quickly than we imagine — like a house that starts returning to nature the moment you pull the front door behind you. Societies that are closed down are difficult to restart; some parts may never revive. An economy does not, as many Keynesians seem to think, run like an old-fashioned railway, operable from innumerable signal cabins, where levers are pushed and pulled by fat controllers to direct the rail traffic safely around the system. An economy is a living organism, in some ways resembling its human quotient in that it is driven by desire, hope, love, aspiration, greed, ambition and a thousand other intangibles that together present an inscrutable front to even the most educated observer. There is no evidence that any of this was taken into account before the lockdown policy was plucked from Xi Jinping’s communist backside.
It is hardly a surprise that human creations, such an economies and societies, come to resemble in nature and inclination their constituent denizens. To restrict the free movement of people through the places they have brought into being as their homes is a dangerous matter. Locking people in their houses may momentarily stop a virus in its tracks, but to believe that this can do anything significant to diminish its inevitable and ineluctable impact is hubristic and ignorant. Such arrogation of godly powers to mere humans is all but guaranteed to backfire, creating repercussions of its own that may be far more serious than what would have transpired naturalistically. As Peter Hitchens puts it, you might as sensibly propose demolishing your house to get rid of the wasp’s nest in the attic.
The reality is that even the most fanatical of its devotees will in the future be unable to say more to the credit of lockdown than that it was a well-intentioned experiment that not merely failed but produced all kinds of counter-productive and foreseeable but unforeseen collateral consequences. Right now, however, sundry authorities seem intent upon ignoring all the evidence in order to pursue whatever agendas remain to be executed in the Time of Covid, which may have no more than begun. Lockdown was an untested hypothesis, unfazing to Chinese communists but less so to the peoples of Western democracies, which will shortly have to begin picking up the pieces. The pandemic of lying that has accompanied these events appear to have lulled the public into believing that, really, all that is happened is a temporary break in proceedings, a bit like a bank holiday weekend that happened to last for a year.
It will, for certain, prove more problematic than that. As Lord Jonathan Sumption has dryly observed, it is relatively easy for a democratic country to turn itself into China, but not so easy to go back to the way things were before.